
A version of this article first appeared in Emily Oster’s newsletter, ParentData.
The school reopening debate continues. A number of large school districts have made decisions —mostly to move to a fully remote schedule— but some are still deciding (like New York), as are many smaller districts and private schools.
Fear and anxiety rage amid all the unknowns, but we aren’t totally flying blind: Summer camps and others child care settings are valuable sources of information on what to expect school reopens. In the service of this, I (with some help from my colleagues at COVID-Explained) have been trying to aggregate information. Here is some of what I think we are seeing, triangulating from several sources.
It’s important to be clear on what we are looking for in the data. From a decision-making standpoint, the central question is whether these settings are sources of outbreaks. That is: If we open schools, will they contribute to spread, make it worse, raise the “R0” value we hear so much about? (That’s the reproductive rate of the virus—the measure of how many people each infected person infects.)
This is different from the question of whether people in schools will have COVID-19. As I’ve written about recently elsewhere, when we open schools, we should expect some cases. The rates in the school will mirror the community even if schools do not contribute to spread at all. This is a reason, in my view, to limit opening to places where the virus levels are lower. (No, I do not have an exact cutoff, but here’s a link to some people who do.) But it’s also a reason to focus in the data on looking for outbreaks, not single cases.
The ideal way to identify outbreaks, from a data standpoint, would be if every child care setting—camp, child care center, etc.—were required to report their enrollment and any COVID-19 cases regularly (say, once a week). Perhaps they could also indicate any precautions they are taking. This could be coordinated by states or, better yet, the Centers for Disease Control and Prevention. It would give us a complete picture of what is going on.
But there is nothing like this. So today I’m going to talk through three imperfect pieces of information and see how we can extrapolate. Specifically, we’ll talk about:
1. Information I’ve crowd-sourced from camps and child care settings
2. Media reports on outbreaks
3. State-reported data
I’ll sum up at the end—at least what I take from this. No TL;DR here since I think we should all draw our own conclusions.
First, the crowd-sourced information. A couple of months ago, fueled by coffee and frustration, I started an effort to collect information from open child care settings on outbreaks. A piece of this effort has involved tracking locations over time, looking at their enrollment and cases by week. (Big thanks to—among others—people at the YMCA, the American Camp Association, and Winnie.com for their help on recruitment.)
Effectively, I’m attempting to generate a voluntary, crowd-sourced sample that would approach what I describe as the ideal above. However, this approach is far from the ideal. The problem is not so much that it is not universal—that’s an inevitable part of sampling—but that it’s not random. Places with COVID-19 outbreaks may be less likely to participate. More generally, the places that want to engage on an effort like this are likely those that are taking other precautions about COVID-19. For all of these reasons, the numbers generated by this approach are likely to understate what we’d see in a random sample.
You may ask (people have) why bother working with this data given its issues. I can see a few reasons. The first is to match anecdote with anecdote. The media coverage (more on this below) can give one the impression that it is impossible to operate a child care setting without outbreaks. The data I have collected contradicts this.
Second, by tracking the same place over time, we can see how common it is for a single case to turn into an outbreak. And, finally, this is an opportunity to see what methods these settings are using as prevention.
What are we seeing? First, if you want to access all the (de-identified) raw data, you can see it here. Enjoy!
To summarize: The case numbers are limited. Among more than 11,500 students and 3,800 staff in the most recent week, for example, there were two student cases and one staff case. The camps—at least some of which are large overnight camps—showed similarly low numbers. In the Google sheet, we can focus on places in hotspots, and the rates are still low.
Again, I am not saying these are the average rates for all organizations. But what we do see is that it is possible to run, for example, a large overnight camp in Texas without any cases of COVID-19. We also see is that there are places that have one or two cases in a week and then do not have cases the following week. Effectively, we see containment.
In the most recent week, I asked locations what they are doing to prevent COVID-19. Ninety percent of the locations contributing data are doing routine temperature checks (note that many states require this) and 73 percent are doing symptom tracking (again, often required). More notable, about 15 percent of the sample is doing some routine testing of either staff or students. These numbers reflect good compliance, and may be part of what has kept cases down in this, again, un-random sample.
In a sense, the polar opposite of the crowd-sourced data is media reports on outbreaks. I say this because these focus only on settings with cases—stories of camps with no cases are not interesting.
Still, this provides a different kind of evidence. It tells us about what can happen in the other direction, the bad direction.
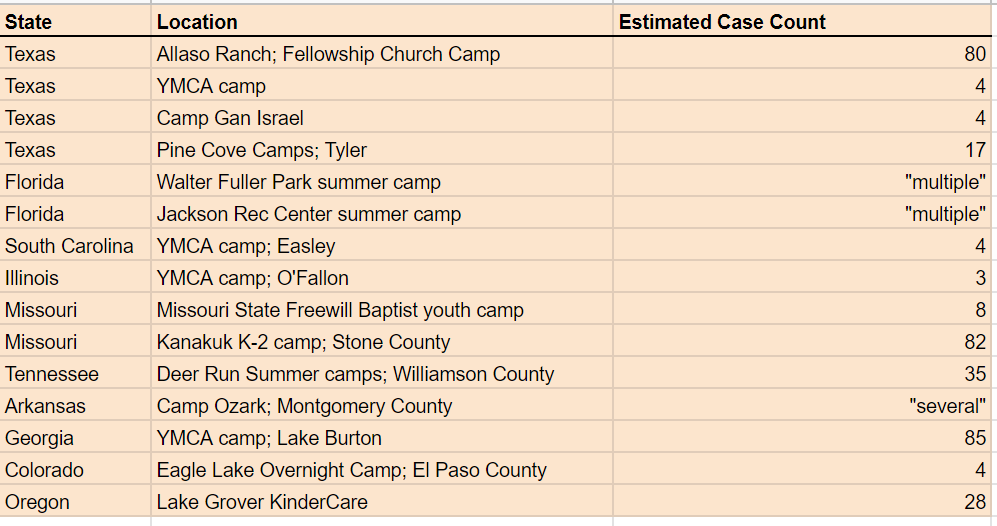
It’s difficult to be comprehensive about outbreaks reported in the media. We sourced from Twitter, from online searches, from various threads. To make it easy to see, we put it in a table, with some key information added. (The table with sources is here.)
{kind=link}
An important note here is that we found additional media stories reporting on a camp or child care closing due to one case among staff, or reporting the presence (or suspected presence) of a case. We did not include these in the table for the simple reason that one case isn’t an outbreak. We focused on cases where there were more than two cases noted.
Some of the outbreaks we found are very small—three or four cases in a setting, with limited details provided. There are, however, several notable, larger outbreaks. Some of these seem inevitable. One location—a camp at Allaso Ranch, in Texas—posted Instagram photos showing large, indoor gatherings with singing and no masks. Given the overall COVID-19 levels in Texas and what we know about indoor unmasked singing events, it is not surprising that an outbreak happened there.
But there are other examples where the outbreak seems less explicable. In one case—the Lake Grove, Oregon, KinderCare—there were a large number of cases in both staff and children and (based on some digging we did) it doesn’t seem like the location did anything objectively “wrong.” It would be helpful if we knew more about these situations, although I think it’s understandable that privacy concerns limit how much locations want to reveal.
The last thing I’ve been looking at is the data that states have been publishing. We’re doing this analysis over at COVID-Explained, and you can see the whole messy disaster here. This data mostly focuses on child care facilities, not camps, but it’s a bit of a hodge-podge.
A challenge with the data provided from many states it is that it provides no ability to look at outbreaks as distinct from cases. For example, California reports out cases linked to child care centers, but they do not provide evidence on clustering of cases. You’d expect some base rate of cases in these settings, but without knowing if the cases are clustered, there’s not sufficient information to know whether child care centers are driving outbreaks.
There are a few states that specifically focus on outbreak data. Colorado reports all clusters of two or more cases within 14 days as outbreaks; their data shows seven child care facility outbreaks since the start of the pandemic, mostly with very small case numbers. North Carolina reports ongoing clusters here, and its most recent update includes 14 clusters, with case counts ranging from five to 14. Oregon does a similar type of reporting and has two clusters identified, one of which is that larger Lake Grove KinderCare case we talked about above.
The random nature of this reporting, the fact that much of it must be dug out of newspaper articles, is not great. But more data is better, even if we cringe a bit at the quality.
Ultimately, the idea is to pull these data together and extrapolate—at least a bit—what we might see in schools. I think there is both bad news and good news here.
On the bad news side, the fact that we see some outbreaks here tells me that it is not realistic to expect no school outbreaks at all. In some cases, the large outbreaks cited above seem clearly linked to behaviors we’d hope schools would avoid, but it is simply not realistic to expect zero clusters of cases to emerge. Some of these could be large.
But on the positive side: Many child care centers and camps, even large ones and even in high-prevalence areas, are operating without significant outbreaks. They are dealing with cases without having them turn into clusters. We see this in the crowd-sourced data. We can also infer it, to some extent, from the media reports and state-level data. The number of clusters observed is simply very limited relative to the overall population.
It’s easy to forget the denominator, but estimates suggest in the range of 5,000 summer camps are operating this summer, including perhaps 1,500 overnight camps. The number of child care centers in the U.S. is in the hundreds of thousands. Yes, it is concerning that there are 14 child care locations in North Carolina with clusters, but this is out of a total of about 6,500 locations, so 0.2 percent.
Again, this doesn’t mean that there aren’t individual cases at other centers—we know there are—but the cluster rate seems limited. Some people will say it is not responsible to open schools if there is going to even one cluster. If we take that approach, this data is not good news, and I think it would realistically say we need to stay closed.
A different approach would be to say that these data suggest the risk of a cluster is fairly small, and focus on opening in states with low case rates, with a key set of procedures in place for limiting spread when individual cases do crop up.
But everyone, cautious or not, should leave this conversation with the sinking feeling that our data isn’t good enough, and that it would be great if I were not the one collecting it.
If you want to help improve the data, here are three action items:
1. If you are a camp/school/child care center and want to be part of the tracking, the baseline survey is here. If you think you can connect me more broadly, please email.
2. If you know of outbreaks I missed, submit information here.
3. If you can help me with better state data, please email.
Finally: As we go into the fall, if any schools do open in person, we need more systematic data collection. My sense is the approach of newsletter-lady-armed-with-Google-Forms could be improved on.
Future Tense is a partnership of Slate, New America, and Arizona State University that examines emerging technologies, public policy, and society.